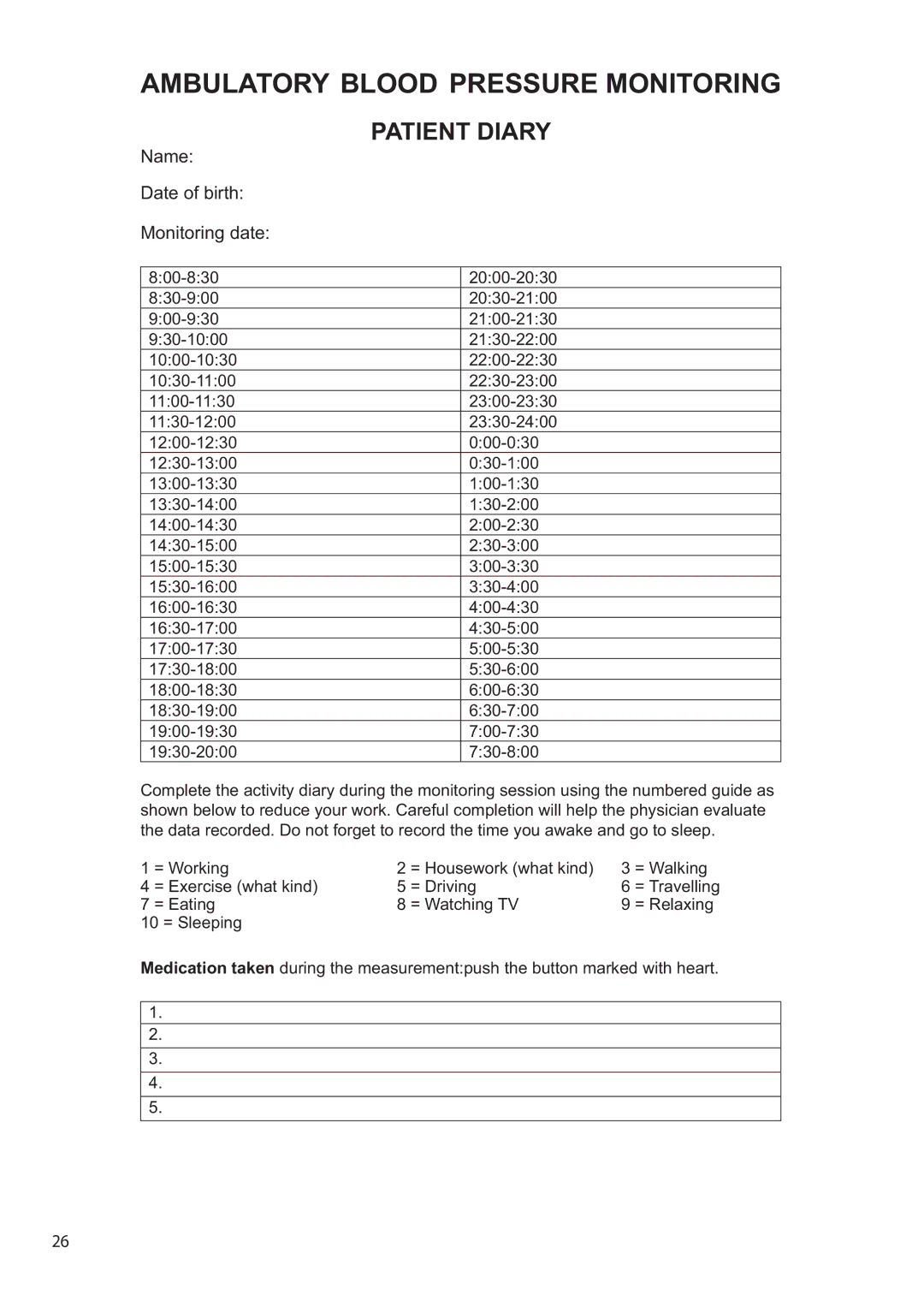
AMBULATORY BLOOD PRESSURE MONITORING
Name: | PATIENT DIARY | |
|
| |
Date of birth: |
|
|
Monitoring date: |
|
|
|
|
|
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
| ||
Complete the activity diary during the monitoring session using the numbered guide as shown below to reduce your work. Careful completion will help the physician evaluate the data recorded. Do not forget to record the time you awake and go to sleep.
1 | = Working | 2 | = Housework (what kind) | 3 | = Walking |
4 | = Exercise (what kind) | 5 | = Driving | 6 | = Travelling |
7 | = Eating | 8 | = Watching TV | 9 | = Relaxing |
10 = Sleeping
Medication taken during the measurement:push the button marked with heart.
1.
2.
3.
4.
5.
26