PARTNER® Advanced Communications System
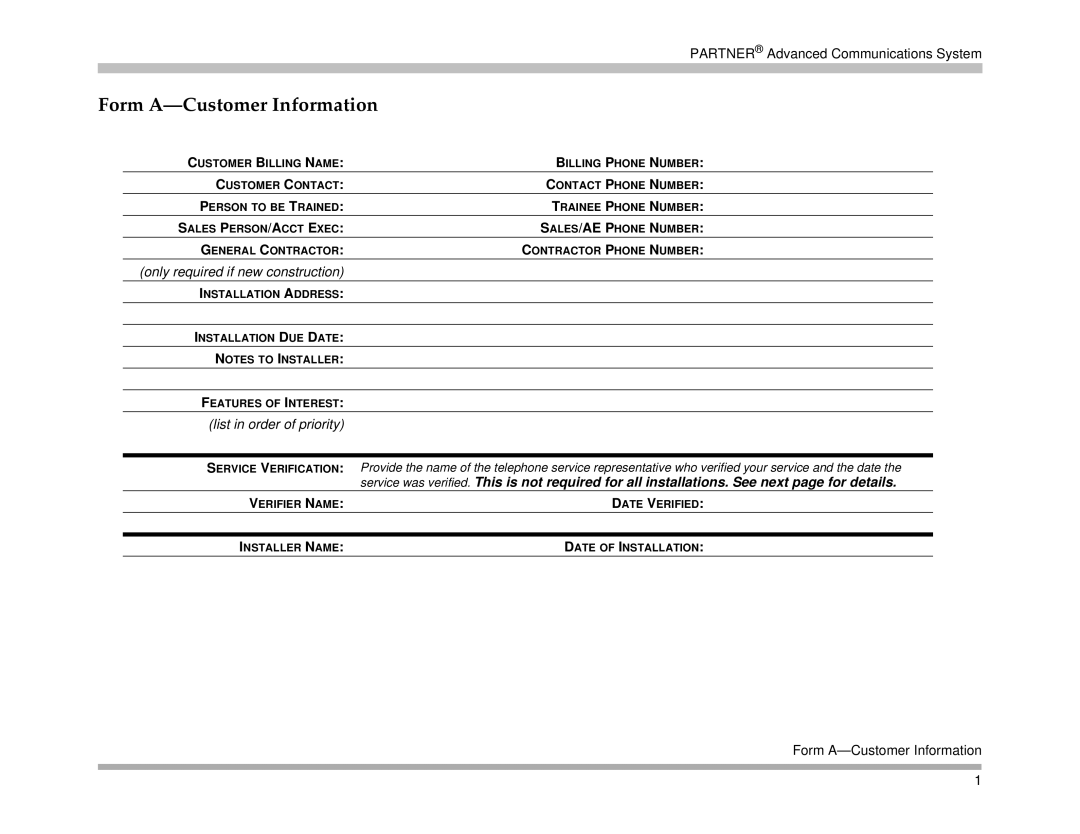
Form A—Customer Information
CUSTOMER BILLING NAME: | BILLING PHONE NUMBER: |
CUSTOMER CONTACT: | CONTACT PHONE NUMBER: |
PERSON TO BE TRAINED: | TRAINEE PHONE NUMBER: |
SALES PERSON/ACCT EXEC: | SALES/AE PHONE NUMBER: |
GENERAL CONTRACTOR: | CONTRACTOR PHONE NUMBER: |
(only required if new construction) |
|
INSTALLATION ADDRESS: |
|
|
|
INSTALLATION DUE DATE: |
|
NOTES TO INSTALLER: |
|
|
|
FEATURES OF INTEREST: |
|
(list in order of priority) |
|
|
|
SERVICE VERIFICATION: | Provide the name of the telephone service representative who verified your service and the date the |
| service was verified. This is not required for all installations. See next page for details. |
VERIFIER NAME: | DATE VERIFIED: |
|
|
INSTALLER NAME: | DATE OF INSTALLATION: |
Form
1