✂LINE. DOTTEDALONG
CUTCUSTOMER:
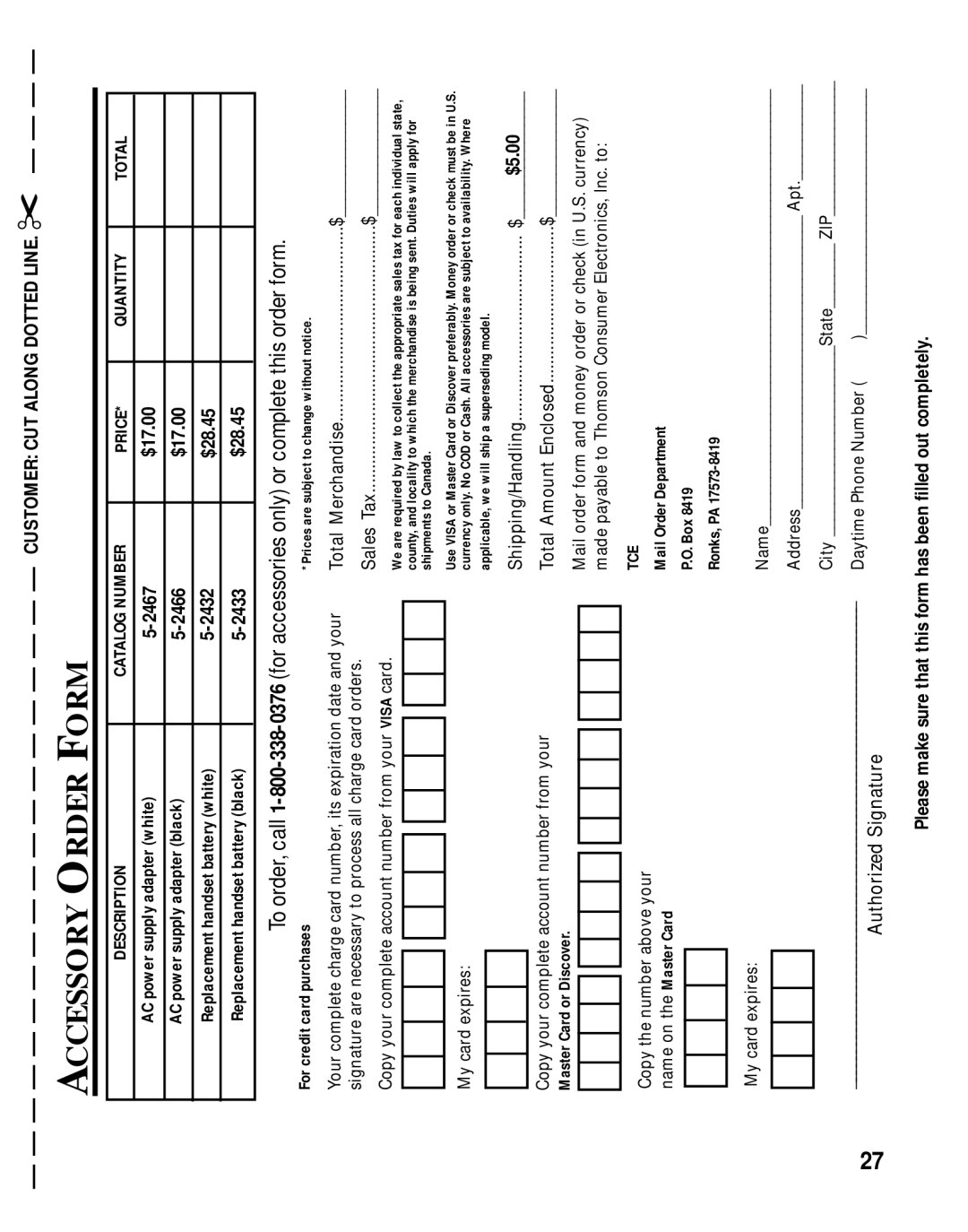
FORM
ORDER
ACCESSORY
TOTAL |
|
|
|
|
|
|
|
|
|
QUANTITY |
|
|
|
|
|
|
|
|
|
PRICE* | $17.00 | $17.00 | $28.45 | $28.45 |
|
|
|
|
|
CATALOGNUMBER |
|
|
|
|
|
|
|
|
|
DESCRIPTION | ACpowersupplyadapter(white) | ACpowersupplyadapter(black) | Replacementhandsetbattery(white) | Replacementhandsetbattery(black) |
|
|
|
|
|
To order, call
*Prices are subject to change without notice.
For credit card purchases
Merchandise.........................................$_______________
Total yourand
dateexpiration
completeYour cardcharge number, its
Sales Tax........................................................$_______________
signature are necessary to process all charge card orders.
Wearerequiredbylawtocollecttheappropriatesalestaxforeachindividualstate, county,andlocalitytowhichthemerchandiseisbeingsent.Dutieswillapplyfor shipmentstoCanada. | UseVISAorMasterCardorDiscoverpreferably.MoneyorderorcheckmustbeinU.S. currencyonly.NoCODorCash.Allaccessoriesaresubjecttoavailability.Where applicable,wewillshipasupersedingmodel. |
CopyyourcompleteaccountnumberfromyourVISAcard. |
|
| Mycardexpires: |
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
| |||
|
|
$5.00_______________
$.......................................
Shipping/Handling
TotalAmountEnclosed.................................$_______________ | Mailorderformandmoneyorderorcheck(inU.S.currency) madepayabletoThomsonConsumerElectronics,Inc.to: | TCE | MailOrderDepartment | P.O.Box8419 |
|
|
| Name_______________________________________________________ | AddressApt.____________ | CityState ZIP_________________ | DaytimePhoneNumber( )_______________________________ |
| ||
Copyyourcompleteaccountnumberfromyour MasterCardorDiscover. |
|
| Copythenumberaboveyour | nameontheMasterCard |
|
|
|
|
| Mycardexpires: |
|
| ____________________________________________________________________ | AuthorizedSignature |
|
|
|
|
|
|
|
|
| ||||||
|
|
|
|
|
|
|
|
| ||||||
|
|
|
|
|
|
|
|
| ||||||
|
|
|
|
|
|
|
|
| ||||||
|
|
|
|
|
|
|
|
| ||||||
|
|
|
|
|
|
|
|
| ||||||
|
|
|
|
|
|
|
|
| ||||||
|
|
|
|
|
|
|
|
| ||||||
|
|
|
|
|
|
|
|
|
| |||||
|
|
|
|
|
|
|
|
| ||||||
|
|
|
|
|
|
|
|
|
| |||||
|
|
|
|
|
|
|
| |||||||
|
|
|
|
|
|
|
|
|
| |||||
|
|
|
|
|
|
|
|
|
| |||||
|
|
|
|
|
|
|
|
|
| |||||
Please make sure that this form has been filled out completely.
27