✂LINE. DOTTEDALONG
CUTCUSTOMER:
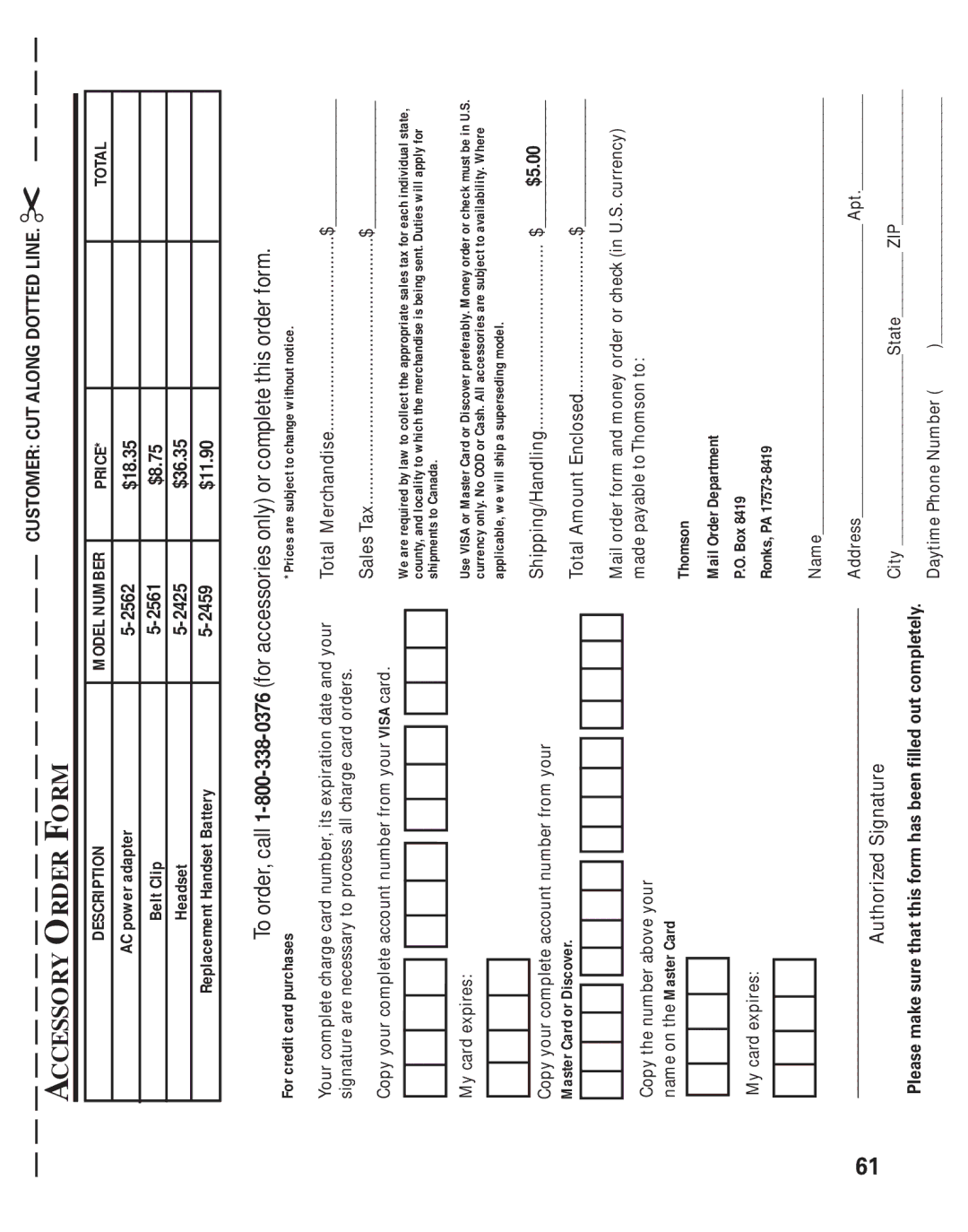
![]() FORM
FORM
![]() ORDER
ORDER
![]() ACCESSORY
ACCESSORY
TOTAL
|
|
|
|
| orcompletethisorderform. |
PRICE* | $18.35 | $8.75 | $36.35 | $11.90 | |
|
|
|
|
| (foraccessoriesonly) |
MODELNUMBER | |||||
|
|
|
|
| |
DESCRIPTION | ACpoweradapter | BeltClip | Headset | ReplacementHandsetBattery |
|
*Prices are subject to change without notice.
For credit card purchases
.........................................MerchandiseTotal $_______________ | ........................................................TaxSales $_______________ | appropriatethecollecttolawbyrequiredareWe salestaxforeachindividualstate, merchandisethewhichtolocalityandcounty,isbeingsent.Dutieswillapplyfor Canada.toshipments |
|
| preferably.DiscoverorCardMasterorVISAUse MoneyorderorcheckmustbeinU.S. accessoriesAllCash.orCODNoonly.currencyaresubjecttoavailability.Where model.supersedingashipwillweapplicable, |
|
|
| .......................................Shipping/Handling$_______________ | .................................EnclosedAmountTotal $_______________ | ||||||
|
|
|
|
|
|
|
|
|
| $5.00 |
|
|
| |||
Yourcompletechargecardnumber,itsexpirationdateandyour signaturearenecessarytoprocessallchargecardorders. |
| CopyyourcompleteaccountnumberfromyourVISAcard. |
|
|
|
| Mycardexpires: |
|
|
|
|
| Copyyourcompleteaccountnumberfromyour | MasterCardorDiscover. |
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||
|
|
|
|
|
|
|
|
|
|
|
| |||||
|
|
|
|
|
|
|
|
|
|
|
| |||||
|
|
|
|
|
|
|
|
|
|
|
| |||||
|
|
|
|
|
|
|
|
|
|
|
| |||||
|
|
|
|
|
|
|
|
| ||||||||
|
|
|
|
|
|
|
|
| ||||||||
|
|
|
|
|
|
|
|
|
|
|
| |||||
|
|
|
|
|
|
|
|
|
|
|
| |||||
|
|
|
|
|
|
|
|
| ||||||||
|
|
|
|
|
|
|
|
| ||||||||
|
|
|
|
|
|
|
|
|
|
|
| |||||
|
| |||||||||||||||
|
|
|
|
|
|
|
|
| ||||||||
|
|
|
|
|
|
|
| |||||||||
|
|
|
|
|
|
|
|
|
|
|
| |||||
Mailorderformandmoneyorderorcheck(inU.S.currency) | madepayabletoThomsonto: |
| Thomson | MailOrderDepartment | P.O.Box8419 | Name_______________________________________________________ | AddressApt.____________ | |||
| Copythenumberaboveyour | nameontheMasterCard |
|
|
|
| Mycardexpires: |
|
| ____________________________________________________________________ |
|
|
|
|
|
|
| ||||
|
|
|
|
|
|
| ||||
|
|
|
|
|
|
| ||||
|
|
|
|
|
|
| ||||
|
|
|
|
|
|
| ||||
|
|
|
|
|
|
| ||||
|
|
|
|
|
|
| ||||
|
|
|
|
|
|
| ||||
|
|
|
|
|
|
| ||||
|
|
|
|
|
|
| ||||
Authorized Signature
State ZIP_________________ | )_______________________________ |
City________________________ | DaytimePhoneNumber( |
| Pleasemakesurethatthisformhasbeenfilledoutcompletely. |
61